- Research
- Open access
- Published:
Diagnostic accuracy of multi-organ point-of-care ultrasound for pulmonary embolism in critically ill patients: a systematic review and meta-analysis
Critical Care volume 29, Article number: 162 (2025)
Abstract
Background
The clinical presentation of acute pulmonary embolism (PE) can range from mild symptoms to severe shock, circulatory arrest and even death, thereby presenting with a significant high mortality when undiagnosed. Computed tomography pulmonary angiography (CTPA) is the gold-standard imaging modality for diagnosing PE, however, it has several practical limitations and is not widely available in low-income country settings. In this context, point-of-care ultrasound (POCUS) has emerged as a valuable bedside, non-invasive diagnostic tool. This meta-analysis assesses the accuracy of multi-organ POCUS for diagnosing PE in critical care settings.
Study design and methods
We conducted a systematic search of Pubmed, Embase, Scopus and the Cochrane Library databases for studies comparing multi-organ POCUS with CTPA or ventilation-perfusion scans for PE diagnosis in critical care departments. Two reviewers independently completed search, data abstraction and conducted quality assessment with QUADAS-2 tool. Heterogeneity was examined with I2 statistics. We used a bivariate model of random effects to summarize pooled diagnostic odds ratio (DOR), sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR) and summary receiver operating characteristic (SROC).
Results
Four studies met the inclusion criteria, comprising 594 patients. The mean age of participants ranged from 55.2 to 71 years. Prevalence of PE ranged from 28 to 66.2%. CTPA was the primary reference standard used in most studies. Multi-organ POCUS for PE diagnosis demonstrated a pooled DOR of 25.3 (95% CI 4.43–82.9) with a pooled sensitivity of 0.90 (95% CI 0.85–0.94; I2 = 0%) and specificity of 0.69 (95% CI 0.42–0.87; I2 = 95%). The PLR was 3.35 (95% CI 1.43–8.02) and the NLR was 0.16 (95% CI 0.08–0.32). The SROC curve showed an AUC of 0.89 (95% CI 0.81–0.94).
Conclusions
Multi-organ POCUS has high diagnostic accuracy for PE diagnosis in critically ill patients. Further research is needed to validated these findings across different patient populations.
PROSPERO registration
CRD42024614328.
Graphical abstract

Background
The clinical presentation of acute pulmonary embolism (PE) can range from mild symptoms to severe shock, cardiac arrest and even death [1,2,3]. Common symptoms include sudden onset dyspnea, chest pain, syncope, and hemoptysis, with dyspnea being the most frequently reported symptom, occurring in a significant majority of patients [2]. This heterogeneity in presentation can be attributed to several factors, such as underlying cause of PE, location and load of thrombus, number of pulmonary lobes affected and the presence of comorbidities [4, 5]. These factos makes the diagnosis of PE challenging, requiring an accurate diagnostic process with a high level of clinical suspicion and a structured stepwise approach. Owing to the nonspecific nature of symptoms and signs, clinical prediction rules such as the Wells score, revised Geneva score, and Pulmonary Embolism Severity Index (PESI) can assist in risk stratification and guide decisions regarding further diagnostic testing [1].
Computed tomographic pulmonary angiography (CTPA) is considered the gold standard for PE diagnosis because of its high sensitivity and specificity [6]. However, the CTPA has several practical limitations in austere scenarios, such as with hemodynamically unstable patients and in limited-resource settings, which can affect its utility. These include high cost, the logistical challenges of transporting an unstable patient to the radiology department, risk of radiation exposure in pregnant patients and limited availability, particularly in low-income countries.Additionally, the use of iodinated contrast material increases the risk of nephrotoxicity and allergic reactions, especially in patients with pre-existing renal impairment or contrast allergies [4].
When CTPA is not feasible, point-of-care ultrasound (POCUS) has demonstrated its usefulness in clinical practice for ruling in or out PE. Each modality—lung ultrasound, leg vein ultrasonography and focused echocardiography—has been independently shown to be useful and accurate method for confirming the diagnosis of PE [7,8,9,10]. However, despite their utility in specific clinical settings, POCUS of each isolated organ system has relatively low sensitivity. As a result, none of these methods alone can reliably rule-out PE. The application of multi-organ POCUS, which combines lung, cardiac and venous ultrasound, has demonstrated increased diagnostic sensitivity for PE in some studies compared with single-organ approaches [11]. A recent meta-analysis [12] evaluated the accuracy of each organ ultrasound in diagnosing PE, but did not assess the performance of multi-organ POCUS approach. Therefore, we conducted a systematic review and meta-analysis on the accuracy of multi-organ POCUS for diagnosing PE in critical care setting.
Methods
This systematic review and meta-analysis was performed and reported in accordance with the Cochrane Collaboration Handbook for Systematic Review of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines [13, 14]. This meta-analysis involved secondary data from published studies, exempting it from institutional review board approval.
Inclusion criteria
We selected articles assessing the accuracy of combined lung, cardiac and venous (multi-organ) POCUS for the diagnosis of PE. The study population included patients of age ≥ 18 years with suspected PE. Two reference standards for the diagnosis of PE were accepted: CTPA and ventilation/perfusion (V/Q) scan. Moreover, the included studies were required to have a 2 × 2 table of true positive, false negative, true negative, and false positive counts, either extracted from the original article or calculated from other reported information. We excluded preclinical studies, studies including pediatric populations, case reports, conference abstracts, opinion articles, editorials and non-English articles.
Search strategy
A systematic literature search was performed in the following databases: PubMed, MEDLINE/Embase, Scopus and the Cochrane Library. The search strategy included combined terms such as ‘’pulmonary embolism’’, ‘’ultrasound'’ and CTPA/ventilation-perfusion scan-related terms. The detailed string is available in the Supplementary Material. Additionally, a backward search (snowballing) and a forward search (citation-tracking) were conducted for the included articles and relevant literature review. If the required data were not available in the published studies, we contacted the corresponding author to obtain the information.
Study screening and selection
Two authors (R.M. and L.G.) independently screened titles and abstracts and then screened the full texts of the selected articles to identify eligible studies. Any disagreements were resolved through discussion with a third author (R.P). Rayyan.ia [15] software was used to screen, select and exclude duplicate studies.
Data extraction
Each included study was independently scrutinized by two authors (R.M. and L.G.) to obtain the following data: study design, sample size, ultrasonography technique, year, country, median population age, sex proportion, prevalence of PE, diagnosis, reference standard for PE diagnosis, and sensitivity and specificity of multiorgan POCUS for the diagnosis of PE.
Risk of bias assessment
Two authors (R.M. and I.D.) independently performed the Quality Assessment of Diagnostic Accuracy Studies-2 tool (QUADAS-2) [16] to evaluate the risk of bias,which was tailored to suit the review question. Signaling questions were used to assess the following domains: patient selection, index test, reference standard and flow and timing. The risk of bias was assessed across each of the 4 domains and applicability across the first 3 domains. If a study had at least one high-risk domain or two moderate-risk domains, it was rated as having an overall high risk of bias. Disagreements about quality assessment were resolved by consensus by an additional author (L.G.).
Statistical analysis
We performed a meta-analysis of the studies using the reference standard of each study for PE diagnosis. Diagnostic effect measures were obtained from 2 × 2 contingency tables to calculate the sensitivity, specificity, diagnostic odds ratio (DOR), positive likelihood ratio (PLR) and negative likelihood ratio (NLR) with 95% confidence intervals (95% CI). To account for heterogeneity in methodology and demographics across studies, a bivariate random-effects model was used, and forest plots were generated for graphical representation. We constructed summary receiver operating characteristic (SROC) models and calculated the area under the curve (AUC).
We quantified the heterogeneity of the included studies using the inconsistency index (I2). Publication bias was assessed by analyzing funnel plot asymmetry and performing Egger’s test. Statistical significance was assumed for p < 0.05. Statistical analysis was carried out via R software/environment (version 4.4.0, R foundation for Statistical Computing).
Results
Study characteristics
As shown in Fig. 1, the initial search yielded 2688 results. After removing duplicate records and excluding ineligible studies, 16 studies remained for full-text review on the basis of the inclusion criteria. Following further examination, 4 studies were ultimately included, encompassing a total of 594 patients.

PRISMA flow diagram of study screening and selection
The characteristics of the included studies are summarized in Table 1. All studies employed a prospective design. The mean age of participants ranged from 55.2 to 71 years, with the female prevalence varying from 20 to 55%. The prevalence of PE among the study populations ranged from 28 to 66.2%.
CTPA was the primary reference standard used. One study utilized both CTPA and V/Q scan [18]. The main alternative diagnoses observed in addition to PE were, pneumonia, heart failure, COPD, acute coronary syndrome and muscular chest pain. Additionally, one study focused exclusively on patients with COVID-19 [19].
Distinct findings were observed across the included studies for the diagnosis of PE using ultrasound. With respect to lung ultrasound, three studies [11, 18, 19] identified PE by noting subpleural wedge-shaped, triangular, or rounded hypoechoic lesions. One study [19] used two or more subpleural consolidations ≥ 1 cm as the diagnostic criteria for PE. The cardiac ultrasound parameters included in all studies were right ventricle (RV) dilatation, D-shaped interventricular septum and visualization of a thrombus in the right cardiac chambers. Venous ultrasound consistently showed the absence of vein collapse during compression with or without a visible intravascular thrombus, which is indicative of deep vein thrombosis (DVT). A comprehensive list of ultrasound features for PE diagnosis is provided in Table 2.
Quality assessment
Figure 2 illustrates the quality assessment of all included studies evaluated using the QUADAS-2 tool. Overall, the assessment indicated a generally low risk of bias, with one study [19] demonstrating a high risk of bias due to concerns in two domains and high applicability concerns in domain 1. A full description of all four domains for each study is provided in Supplementary Method 2.

Quality assessment of included studies. Overall, the assessment indicated a generally low risk of bias, with one study demonstrating a high risk of bias
The funnel plot (Fig. 3) revealed slight asymmetry upon visual inspection.However, Egger’s regression test could not be conducted because of the limited number of studies included.
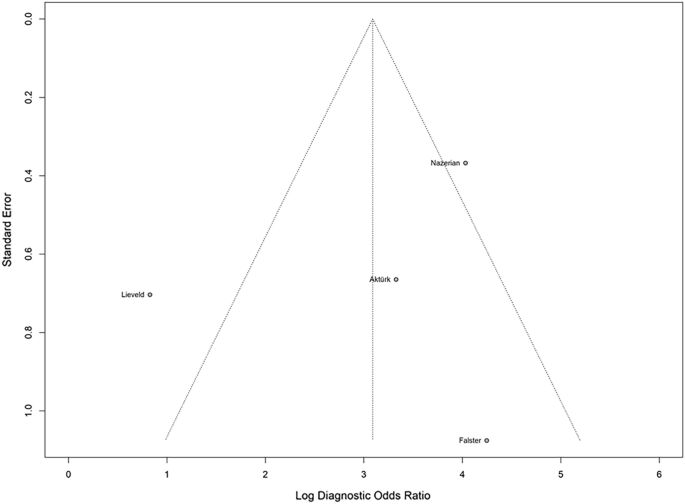
Funnel plot asymmetry test for publication bias using Deek’s model revealed slight asymmetry
Diagnostic accuracy of multiorgan POCUS
Figure 4 presents the summary estimates of sensitivity and specificity for each individual study. These estimates provide insight into the diagnostic performance of multi-organ ultrasound in detecting PE across the included studies. The pooled DOR was 25.3 (95% CI 4.43–82.9). The pooled sensitivity and specificity of the four studies for the diagnosis of PE were 0.90 (95% CI 0.85–0.94; I2 = 0%) and 0.69 (95% CI 0.42–0.87; I2 = 95%), respectively, with a PLR of 3.35 (95% CI 1.43–8.02) and a NLR of 0.16 (95% CI 0.08–0.32).The SROC curve had an AUC of 0.89 (Fig. 5, 95% CI 0.81–0.94). When omitting the study with high risk of bias, the pooled sensitivity was 0.91 (95% CI 0.85–0.94; I2 = 0%), specificity 0.84 (95% CI 0.73–0.90; I2 = 44%), PLR of 5.17 (95% CI 3.5–7.55) and NLR of 0.118 (95% CI 0.07–0.18).

Forest plot of pooled sensitivity (top) and specificity (bottom) of multi-organ point-of-care ultrasound for pulmonary embolism diagnosis
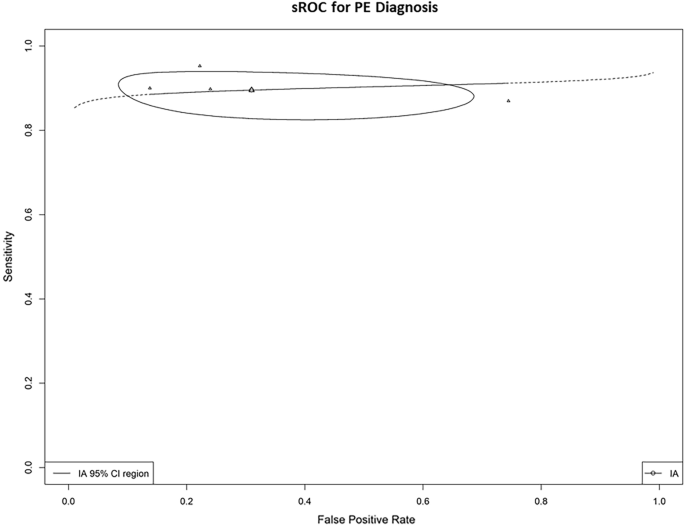
Summary receiver operator curve of diagnostic performance of multi-organ point-of-care ultrasound for pulmonary embolism diagnosis. PE: pulmonary embolism
Sensitivity analyses
In the leave-one-out sensitivity analyses, the overall pooled sensitivity remained stable across different iterations of the meta-analysis with individual studies omitted (Supplementary Fig. 1). The overall specificity also showed consistent values across interactions, however,there was a significant decrease in heterogeneity (I2 = 44%) when one specific study was excluded [18].
Discussion
In this meta-analysis encompassing 594 patients from 4 studies, we evaluated the diagnostic accuracy of multi-organ POCUS for PE in critical care setting. The results demonstrated a DOR of 25.3 with a pooled sensitivity and specificity of 90% and 69%, respectively. Additionally, the SROC curve revealed an AUC of 0.89, indicating high test accuracy. To our knowledge, this is the first meta-analysis assessing the accuracy of a multi-organ POCUS approach—combining lung, cardiac and venous ultrasound- for the diagnosis of PE in critically ill patients.
PE is a common and potentially fatal condition if left untreated [1, 20]. Consequently, the diagnostic approach must be both efficient and judicious, balancing the need to avoid unnecessary testing while ensuring timely diagnosis and treatment to reduce morbidity and mortality.
The latest European Society of Cardiology guidelines [21] suggest that the optimal diagnostic strategy to confirm or exclude PE involves a combination of pretest probability assessment using validate tools such Wells score or the Geneva score, plasma D-dimer measurement and CTPA. While CTPA is currently regarded as the gold-standard diagnostic method, it has several limitations, including high cost, lack of 24-h availability in many hospitals, particularly in limited-resource settings, and the need for patient transportation to the radiology department.This latter requirement poses a significant risk in hemodynamically unstable patients. These factors, in addition to presenting risks inherent to the method, such as radiation exposure and potential allergic reactions to contrast agents, can make PE diagnosis challenging in the critically ill patients. Given these challenges, POCUS has emerged as a valuable diagnostic tool. It is non-invasive, widely available and can be performed at the bedside by the treating physician. Lung ultrasound, which can detect sonographic signs of pulmonary infarction, has been validated and is recommended by experts as a promising alternative when CTPA is not feasible [22]. The use of lung ultrasonography in emergency (BLUE) protocol was the first dual-organ ultrasound approach, combining lung and venous ultrasound, and demonstrated a sensitivity of 81% and a specificity of 99% for PE diagnosis [23].
Despite its advantages, ultrasound assessments typically have limited utility in conclusively ruling out PE due to their relatively low sensitivity, even under optimal insonation conditions. To address this limitation, Nazerian et al. [11] introduced a multi-organ POCUS approach that integrates cardiac, lung and venous ultrasound with the Wells score and D-dimer testing. This approach demonstrated promising potential for ruling out PE and may serve as a valid alternative when CTPA is unavaliable or contraindicated.
Previous meta-analyses evaluating the accuracy of ultrasound for PE diagnosis have primarily focused on single-organ insonation or dual-organ protocols [10, 24–26]. The potential to enhance the accuracy of a multi-organ POCUS approach lies in its ability to improve sensitivity—combining negative findings from lung, cardiac, and venous ultrasounds yields a higher negative predictive value than any single-organ ultrasound alone. POCUS may be charged by the crucial role of becoming the valid alternative to CTPA. Furthermore, incorporating likelihood ratios into pretest probability assessments and integrating multi-organ POCUS with clinical prediction tools, such as the Wells score, has been shown to enhance diagnostic efficiency. This approach has the potential to significantly reduce the number of unnecessary CTPA scans in emergency settings [27]. Another study published by Falster and colleagues [28] demonstrated a substantial reduction in referral do diagnostic imaging in suspected PE when a multi-organ POCUS approach was employed. Therefore, extending the ultrasound assessment to multiple organs may further improve the accuracy of pretest probability calculations, making the multi-organ POCUS approach a valuable and potentially a cost-effective diagnostic strategy.
This review has several strengths. To our knowledge, this is the first meta-analysis to evaluate the accuracy of a combined lung, cardiac and venous POCUS approach in ruling-in and ruling-out PE, addressing a gap left by previous reviews that focused on single or dual-organ evaluations. Additionally, we implemented a rigorous and comprehensive search strategy across multiple databases, complemented by backward and forward citation tracking. Only prospective studies were included, most of which demonstrated a low risk of bias.
However, our study has also several limitations. First, despite a thorough search and selection process, only four studies met the inclusion criteria. This small sample size may limit the generalizability of the findings and reduce the statistical power to detect smaller effects. Second, significant heterogeneity in specificity could affect the applicability of the results. Notably, the leave-one-out sensitivity analysis revealed a marked decrease in heterogeneity in the specificity plot when the study by Lieveld et al. was excluded. This particular study focused exclusively in COVID-19 population, which has a greater risk for both PE and other lung [29] and cardiac ultrasound [30] findings that could mimic PE, leading to elevated false-positive rates. Moreover, the lung ultrasound criteria for diagnosing PE in this study were not specific (Table 2) as evidenced by its notably low specificity of 25%, which contrasts sharply with the findings of other studies. Third, it is important to consider the characteristics of the study populations included in our meta-analysis. Notably, three out of the four studies included were conducted in emergency department (ED) settings. This predominance of ED-based studies could introduce bias, potentially skewing the diagnostic performance of POCUS in favor of more favorable PLRs and NLRs. As a result, the accuracy reported in our meta-analysis may be optimized for acute, high-suspicion clinical scenarios rather than for routine or lower-suspicion settings. Finally, variability in ultrasound equipment and operator expertise across the included studies could also influence diagnostic accuracy. These factors should be considered when interpreting the results and considering their applicability to broader clinical contexts.
Conclusion
In our study, multi-organ POCUS has demonstrated high accuracy for ruling in or out PE in critically ill patients, offering a valuable, cost-effective alternative to traditional imaging modalities, especially in resource-limited environments. Further research is needed to validated these findings across different patient populations.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- CTPA:
-
Computed tomographic pulmonary angiography
- DOR:
-
Diagnostic odds ratio
- DVT:
-
Deep vein thrombosis
- I2 :
-
Inconsistency index
- ITT:
-
Intention-to-treat
- NLR:
-
Negative likelihood ratio
- PE:
-
Pulmonary embolism
- PLR:
-
Positive likelihood ratio
- POCUS:
-
Point-of-care ultrasound
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analysis
- QUADAS-2:
-
Quality assessment of diagnostic accuracy studies-2
- RV:
-
Right ventricle
- SROC:
-
Summary receiver operating characteristic
- V/Q:
-
Ventilation/perfusion
References
Madsen PH, Hess S. Symptomatology, clinical presentation and basic work up in patients with suspected pulmonary embolism. Adv Exp Med Biol. 2017;906:33–48.
Miniati M, Cenci C, Monti S, Poli D. Clinical presentation of acute pulmonary embolism: survey of 800 cases. PLoS ONE. 2012;7(2):e30891.
Millington SJ, Aissaoui N, Bowcock E, Brodie D, Burns KEA, Douflé G, Haddad F, Lahm T, Piazza G, Sanchez O, Savale L, Vieillard-Baron A. High and intermediate risk pulmonary embolism in the ICU. Intensive Care Med. 2024;50(2):195–208.
Khasin M, Gur I, Evgrafov EV, Toledano K, Zalts R. Clinical presentations of acute pulmonary embolism: a retrospective cohort study. Medicine. 2023;102(28):e34224.
Bikdeli B, Muriel A, Wang Y, Piazza G, Khairani CD, Rosovsky RP, Mehdipoor G, O’Donoghue ML, Madridano O, Lopez-Saez JB, Mellado M, Brasero AMD, Grandone E, Spagnolo PA, Lu Y, Bertoletti L, López-Jiménez L, Núñez MJ, Blanco-Molina Á, Gerhard-Herman M, Goldhaber SZ, Bates SM, Jimenez D, Krumholz HM, Monreal M, RIETE Investigators. Sex-related differences in patient characteristics, risk factors, and symptomatology in older adults with pulmonary embolism: findings from the SERIOUS-PE study. Semin Thromb Hemost. 2023;49(7):725–35.
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, Leeper KV, Popovich J, Quinn DA, Sos TA, Sostman HD, Tapson VF, Wakefield TW, Weg JG, Woodard PK, PIOPED II Investigators. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med. 2006;354(22):2317–27.
Wiener RS, Ouellette DR, Diamond E, Fan VS, Maurer JR, Mularski RA, Peters JI, Halpern SD. An official American Thoracic Society/American College of Chest Physicians policy statement: the Choosing Wisely top five list in adult pulmonary medicine. Chest. 2014;145(6):1383–91.
Du Y, Yang A, Wang X. Accuracy of transthoracic lung ultrasound for diagnosing pulmonary embolism: an updated systematic review and meta-analysis. Thromb Res. 2024;241:109112.
Boccatonda A, Andreetto L, Vicari S, Campello E, Simioni P, Ageno W. The diagnostic role of lung ultrasound and contrast-enhanced ultrasound in pulmonary embolism. Semin Thromb Hemost. 2024;50(6):842–50.
Fields JM, Davis J, Girson L, Au A, Potts J, Morgan CJ, Vetter I, Riesenberg LA. Transthoracic echocardiography for diagnosing pulmonary embolism: a systematic review and meta-analysis. J Am Soc Echocardiogr. 2017;30(7):714-723.e4.
Nazerian P, Vanni S, Volpicelli G, Gigli C, Zanobetti M, Bartolucci M, Ciavattone A, Lamorte A, Veltri A, Fabbri A, Grifoni S. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest. 2014;145(5):950–7.
Falster C, Jacobsen N, Coman KE, Højlund M, Gaist TA, Posth S, Møller JE, Brabrand M, Laursen CB. Diagnostic accuracy of focused deep venous, lung, cardiac and multiorgan ultrasound in suspected pulmonary embolism: a systematic review and meta-analysis. Thorax. 2022;77(7):679–89.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane, 2023.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: a web and mobile app for systematic reviews. Syst Rev. 2016;5:210.
Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36.
Aktürk ÜA, Koçak ND, Ernam D. The role of multi-organ ultrasonography for diagnosing non-massive pulmonary thromboembolism. Biomed Res. 2017;28(18).
Falster C, Egholm G, Wiig R, Poulsen MK, Møller JE, Posth S, Brabrand M, Laursen CB. Diagnostic accuracy of a bespoke multiorgan ultrasound approach in suspected pulmonary embolism. Ultrasound Int Open. 2023;8(2):E59–67.
Lieveld A, Heldeweg MLA, Smit JM, Haaksma ME, Veldhuis L, Walburgh-Schmidt RS, Twisk J, Nanayakkara PWB, Heunks L, Tuinman PR. Multi-organ point-of-care ultrasound for detection of pulmonary embolism in critically ill COVID-19 patients: a diagnostic accuracy study. J Crit Care. 2022;69:153992.
Bĕlohlávek J, Dytrych V, Linhart A. Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Exp Clin Cardiol. 2013;18(2):129–38.
Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, Huisman MV, Humbert M, Jennings CS, Jiménez D, Kucher N, Lang IM, Lankeit M, Lorusso R, Mazzolai L, Meneveau N, Ní Áinle F, Prandoni P, Pruszczyk P, Righini M, Torbicki A, Van Belle E, Zamorano JL, ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543–603.
Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reissig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577–91.
Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure:the BLUE protocol. Chest [Internet]. 2008;134(1):117–25.
Squizzato A, Rancan E, Dentali F, Bonzini M, Guasti L, Steidl L, Mathis G, Ageno W. Diagnostic accuracy of lung ultrasound for pulmonary embolism: a systematic review and meta-analysis. J Thromb Haemost. 2013;11(7):1269–78.
Cao J, Sun J, Wang Y, Wang L. Diagnostic accuracy of cardiopulmonary ultrasound for pulmonary embolism: a systematic review and meta-analysis. Echocardiography. 2022;39(2):185–93.
Kagima J, Stolbrink M, Masheti S, Mbaiyani C, Munubi A, Joekes E, Mortimer K, Rylance J, Morton B. Diagnostic accuracy of combined thoracic and cardiac sonography for the diagnosis of pulmonary embolism: a systematic review and meta-analysis. PLoS ONE. 2020;15(9):e0235940.
Nazerian P, Volpicelli G, Gigli C, Becattini C, Sferrazza-Papa GF, Grifoni S, Vanni S, Ultrasound Wells Study Group. Diagnostic performance of wells score combined with point-of-care lung and venous ultrasound in suspected pulmonary embolism. Acad Emerg Med. 2017;24(3):270–80.
Falster C, Mørkenborg MD, Thrane M, Clausen J, Arvig M, Brockhattingen K, Biesenbach P, Paludan L, Nielsen RW, Nhi Huynh TA, Poulsen MK, Brabrand M, Møller JE, Posth S, Laursen CB. Utility of ultrasound in the diagnostic work-up of suspected pulmonary embolism: an open-label multicentre randomized controlled trial (the PRIME study). Lancet Reg Health Eur. 2024;28(42):100941.
Blazic I, Cogliati C, Flor N, Frija G, Kawooya M, Umbrello M, Ali S, Baranne ML, Cho YJ, Pitcher R, Vollmer I, van Deventer E, Del Rosario PM. The use of lung ultrasound in COVID-19. ERJ Open Res. 2023;9(1):00196–2022.
Sanchez PA, O’Donnell CT, Francisco N, Santana EJ, Moore AR, Pacheco-Navarro A, Roque J, Lebold KM, Parmer-Chow CM, Pienkos SM, Celestin BE, Levitt JE, Collins WJ, Lanspa MJ, Ashley EA, Wilson JG, Haddad F, Rogers AJ. Right ventricular dysfunction patterns among patients with COVID-19 in the intensive care unit: a retrospective cohort analysis. Ann Am Thorac Soc. 2023;20(10):1465–74.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
R.H.M. led the conceptualization, study design, literature search, data extraction, and statistical analysis; he also drafted the manuscript and critically interpreted the results. L.G.P. participated in the literature search, data extraction, quality assessment, and risk of bias assessment. I.D.L. contributed to the literature search, statistical analysis, quality assessment, and risk of bias assessment. A.T.B. was involved in data extraction, statistical analysis, quality assessment, and risk of bias assessment. R.D.H.P. supervised the study, contributed to manuscript drafting, critical interpretation of results, and writing—review and editing. G.V. supervised the study, contributed to manuscript drafting, critical interpretation of results, writing—review and editing, and provided final review and approval of the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Melo, R.H., Gioli-Pereira, L., Lourenço, I.D. et al. Diagnostic accuracy of multi-organ point-of-care ultrasound for pulmonary embolism in critically ill patients: a systematic review and meta-analysis. Crit Care 29, 162 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13054-025-05359-x
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13054-025-05359-x